Discovery & clinical workflow mapping
Operator interviews across the procedure room, clinician hand-off, and PACS/EMR landscape. GDPR + HIPAA posture mapping; tablet ergonomics for sterile-field use.
Case study · HealthTech · Endoscopy
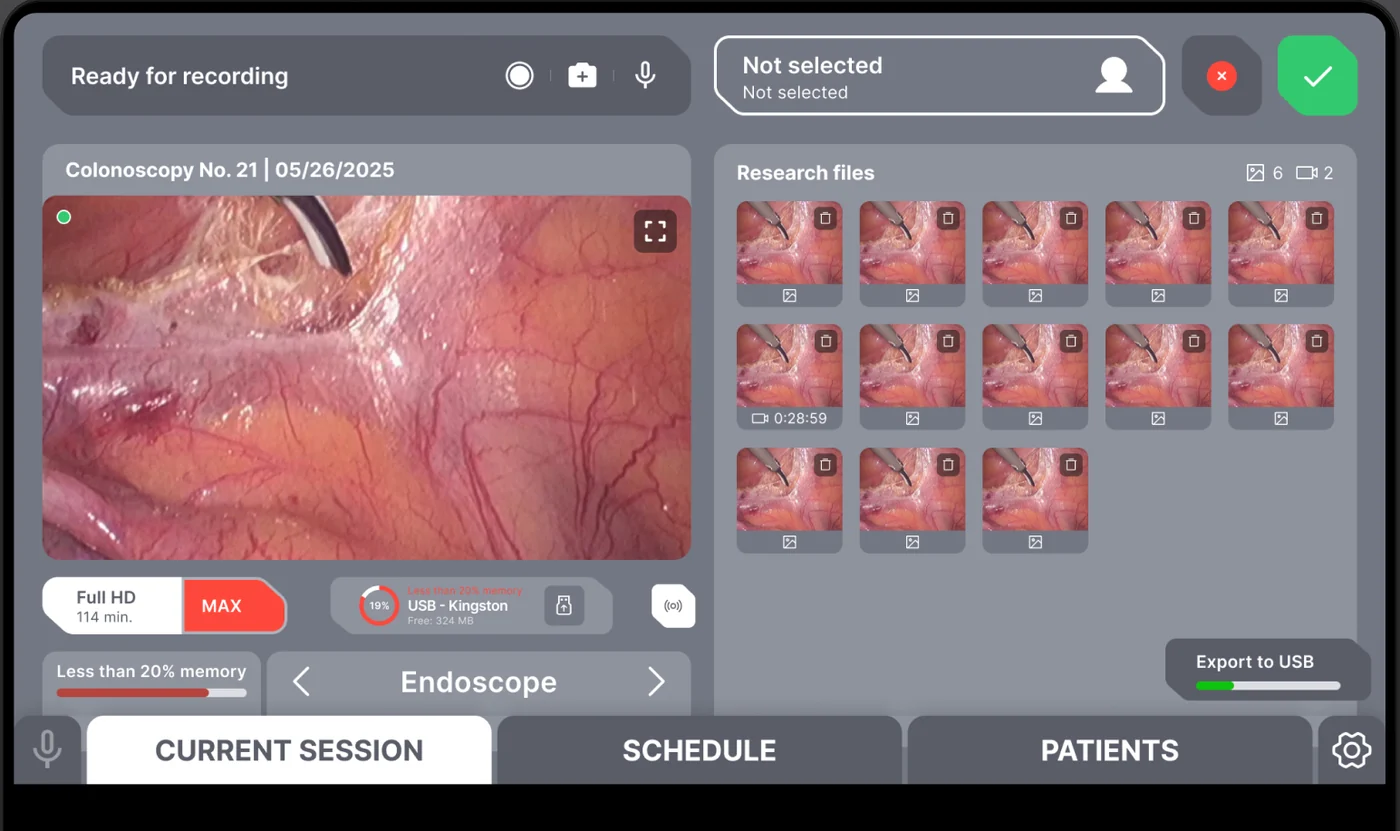
The ArgoView team needed clinical software that did not look or feel like a generic 2010-era EMR plug-in. The product is built for clinicians performing endoscopic procedures — gastroenterology, ENT, pulmonology — and the core insight was that the recording surface has to live on a tablet next to the patient, not on a desktop two rooms away. Operators in the United
The ArgoView team needed clinical software that did not look or feel like a generic 2010-era EMR plug-in. The product is built for clinicians performing endoscopic procedures — gastroenterology, ENT, pulmonology — and the core insight was that the recording surface has to live on a tablet next to the patient, not on a desktop two rooms away. Operators in the United States and the European Union expect a familiar tablet-first interaction model, GDPR-aligned handling of patient data, and an export path that talks DICOM and HL7 to whatever PACS or hospital information system the clinic already runs. We built ArgoView from first principles as a web application: a PHP 8 / Laravel 10 backend, a React + TypeScript front end optimized for iPad and clinical desktops, and a deliberate architectural choice — described below — to move HD video capture out of the backend and into the browser tier so the endoscope camera feed runs at frame rate without queueing through a server.
A snapshot of what the ArgoView build delivered across its first production cycle for the US and EU.
The dominant architectural decision on the ArgoView build was where the HD video feed from the endoscope hardware actually lives in transit. The naive first cut routed the feed through a server-side capture process, transcoded on the backend, and shipped to the React client as an HLS stream. That design failed two acceptance tests immediately: HLS adds two- to six-second latency that is unacceptable for a clinician steering an endoscope, and the backend transcode queue became a hard single point of failure under multi-room load. We rebuilt the capture surface on browser-tier APIs — WebRTC for the live feed and the MediaRecorder API for in-browser frame-accurate capture — and the backend role shrank to durable storage, indexing, and the export pipeline. The resulting tablet-first UX feels native and lets clinicians scrub a recording mid-procedure without leaving the sterile field.
For the United States and the European Union, the second-order benefit of browser-tier capture is that patient video never has to traverse a third-party transcoding stack. We can place the durable-storage tier in an EU data center for European clinics and a US-East region for North American clinics — without introducing a separate codebase per region — while keeping audit-ready logging of every read of the study. The custom software development practice that delivered the platform owns the resulting performance budget end to end.
| Dimension | Browser WebRTC (ArgoView) | Server-side HLS transcode | Native desktop installer |
|---|---|---|---|
| Glass-to-glass latency | Sub-200 ms typical | 2–6 s buffered | Sub-100 ms |
| Install footprint | Zero — opens in Safari / Chrome | Zero — but heavy server fleet | Per-clinic installer + updates |
| Tablet support | First-class on iPadOS | Works but feels slow | Not viable |
| Backend cost at 50 rooms | Storage + index only | Heavy transcode fleet | Light backend |
| PHI traversal surface | Minimal — never hits transcoder | PHI on transcode fleet | Local-only by default |
| Regional placement | Per-region storage tier | Per-region transcode fleet | On-prem only |
| Browser maturity (2024) | Mainline on Safari 14+, Chrome 90+ | Universal | N/A |
Standards references: DICOM Standard, HL7, MDN WebRTC documentation.
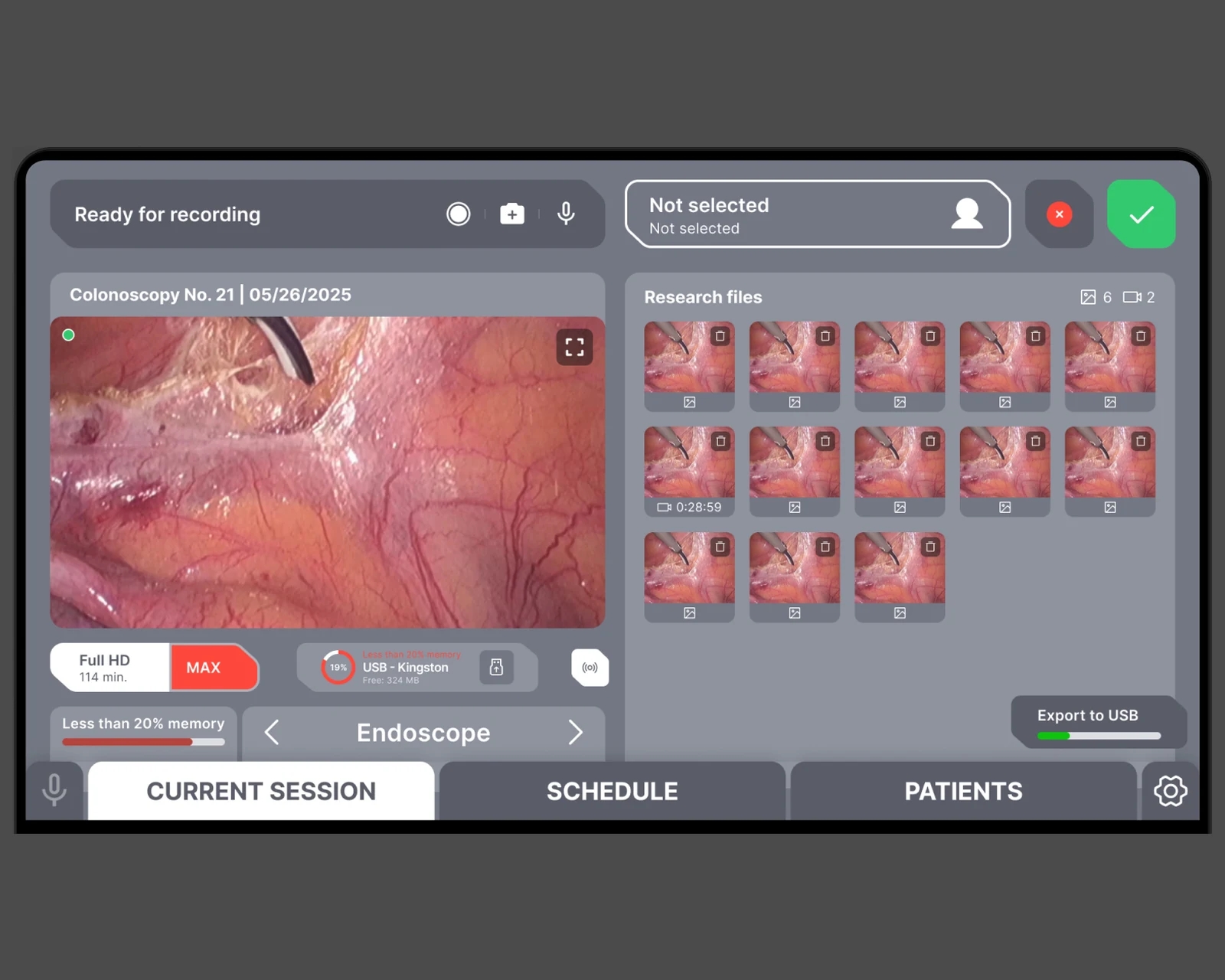
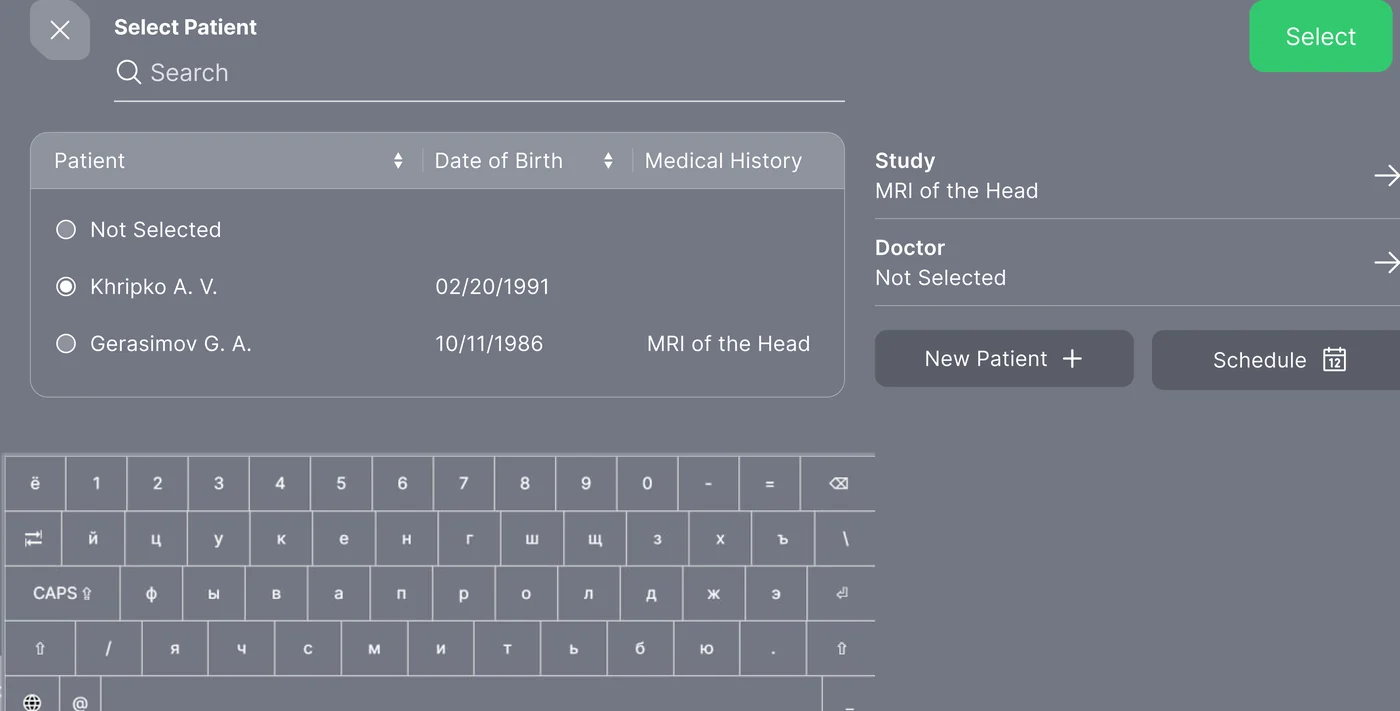
The clinician-facing surface is built in React and TypeScript with a state machine that maps directly to the procedure lifecycle — idle, patient selected, recording, paused, completed, archived. The whole layer is optimized for iPadOS in Safari: large tap targets, single-column flow above 1024 px, and an aggressive offline-first cache so a brief Wi-Fi blip in the procedure room never strands the clinician mid-record. Patient selection lives one tap behind the connect button with a latency-sorted list cached locally so the picker never blocks on a network round-trip. The recording surface itself is one large region with a fixed action bar — record, pause, snapshot, attach to current study — and the recorded clips bind immediately into the patient's study record.
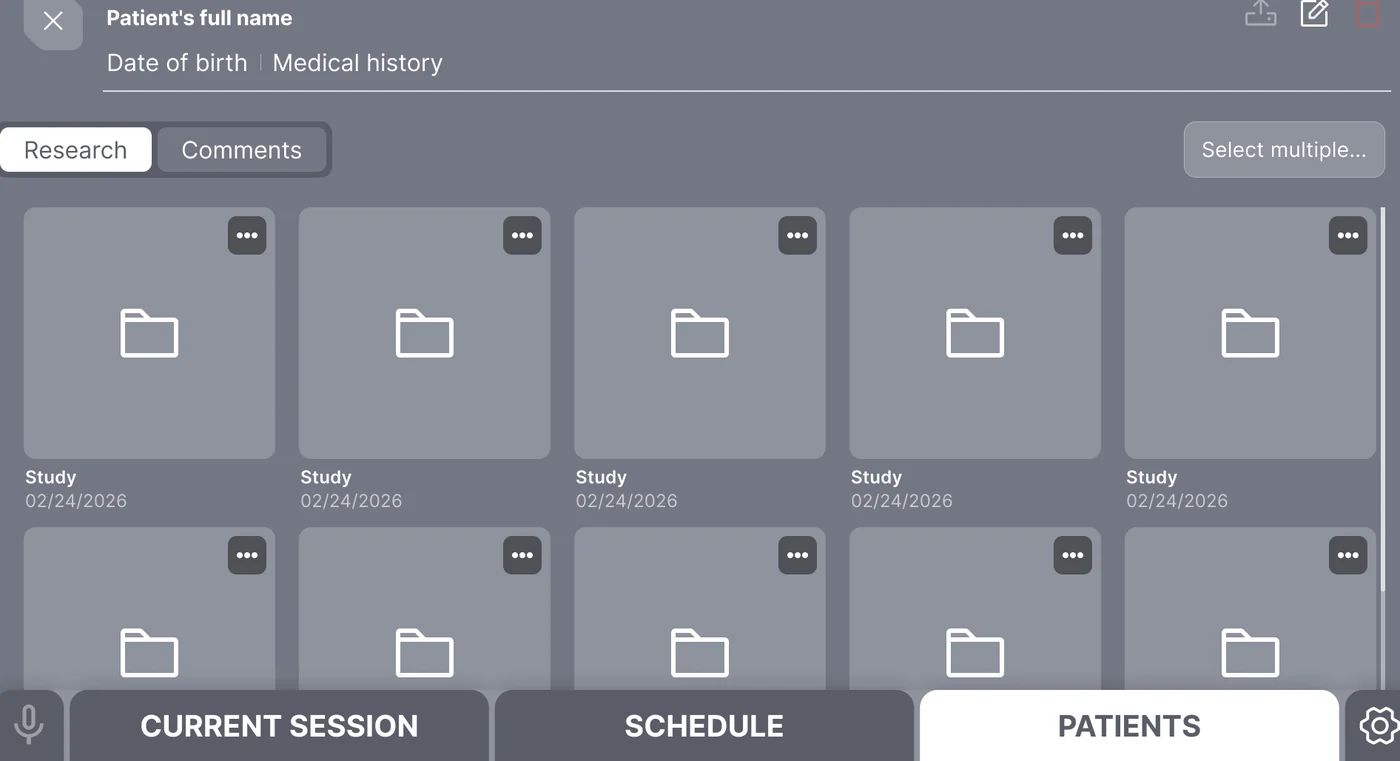
Beyond the live capture, the patient record screen shows the full examination history: prior studies, attached imaging, clinician notes, and the export status for each artifact. Role-based access keeps protected health information narrowly scoped — only assigned clinicians see a given patient's record, every read is logged, and the audit trail is queryable from the admin tier. The same engineering team builds the React surface, the PHP 8 backend, and the in-clinic deployment artifacts as part of our web application development practice.
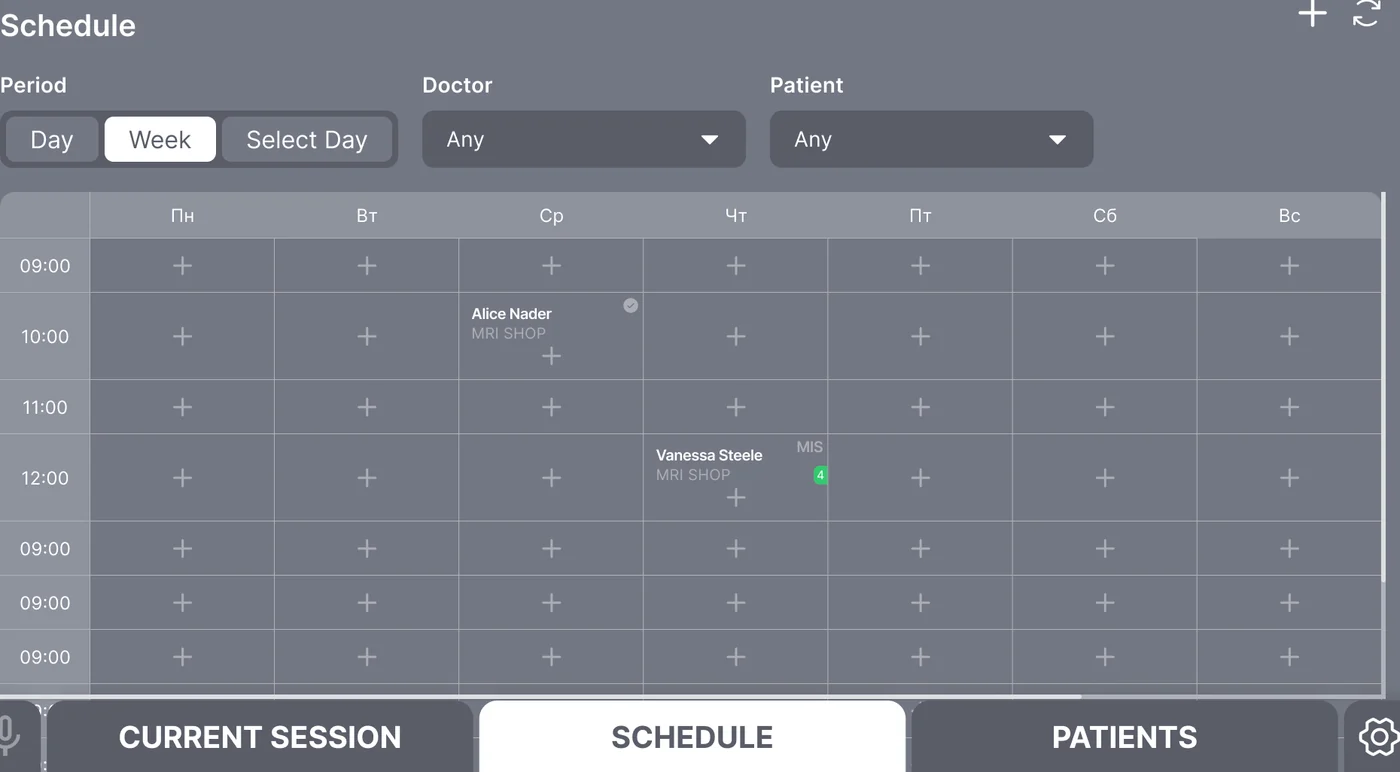
The scheduling subsystem solves the most boring and most important problem in a clinical setting: who is doing what procedure in which room at what time, and who in the clinic can override that schedule when a case runs long. The scheduler runs as a calendar view with clinician swimlanes, drag-and-drop rebooking, and an audit-ready history of every change — who moved which procedure, when, and with what justification. Capacity planning runs in the background: the system flags overlapping bookings, equipment conflicts, and clinician overtime before the conflict reaches the patient. For multi-room clinics in the United States and the European Union, the schedule view is the operational heartbeat of the day — and the audit log behind it is the documentation hospital administrators need.
Hand-off between clinicians is built into the workflow rather than left to a hallway conversation. When a procedure completes, the recording, snapshots, and structured notes attach to the patient record, the export pipeline kicks off in the background, and the next clinician in the room sees a clean idle screen for the next case. Cross-clinic operators in the European Union and the United States use the same scheduling surface against region-specific data tiers without a per-region fork of the code base.
Hospital information systems do not speak HTTP JSON — they speak DICOM and HL7. ArgoView's export pipeline produces DICOM Secondary Capture objects for the still images and DICOM-encapsulated MP4 series for the video studies, with HL7 ORU^R01 messages carrying the structured results back to the ordering EMR. Each export is signed, hashed, and recorded against the originating study so the chain of custody from procedure room to PACS is auditable end to end. For US clinics this matters under HIPAA's documentation requirements; for EU clinics it matters under GDPR right-of-access obligations and the country-specific medical-records statutes that sit on top of it.
The PHI handling posture is enforced at the architecture layer, not just the policy layer. Patient identifiers are stored in a separate schema from the study artifacts, joined through opaque tokens with a short rotation window. Storage encryption is on by default, every read of a patient record writes to the audit trail, and infrastructure-as-code policies prevent accidental introduction of long-lived plaintext identifiers. The posture is built to align with GDPR for the European Union and with CCPA / CPRA obligations for clinics serving residents of California and the wider United States. It is also positioned for HIPAA technical-safeguard mapping when a US deployment requires it.
Compliance posture: GDPR-aligned · ISO 27001 ready · SOC 2 Type II in progress · HIPAA-capable · CCPA-acknowledged.
A five-phase build that took ArgoView from product specification to production across the US and EU.
Operator interviews across the procedure room, clinician hand-off, and PACS/EMR landscape. GDPR + HIPAA posture mapping; tablet ergonomics for sterile-field use.
Browser-tier WebRTC + MediaRecorder choice, Laravel 10 backend skeleton, regional storage tier design, DICOM and HL7 export contract.
React + TypeScript clinician surface optimized for iPadOS; PHP 8 backend with audit-trail-first data model; admin tier for the operator's deployment team.
PHI handling pass, role-based access enforcement, infrastructure-as-code policies that block logging regressions, third-party readiness scaffolding.
Clinic-by-clinic go-live across the US and EU, PACS validation against operator environments, training materials, and on-call hand-off.
ArgoView's licensing model is per-room with a fair-use tier for multi-clinic operators — a structure designed for the way clinical procurement actually buys software in the United States and the European Union, where capital-cost endoscopy hardware drives the budget and software is procured against the device. The entitlement service was built to support that model cleanly: a clinic's seat count, room count, and export quota are configuration values against the entitlement record, not code changes against the application. Reseller and OEM bundling is supported through the same record — an endoscope-hardware vendor that wants to ship ArgoView as part of its device offering can issue branded entitlement tokens that turn on a clinic's seat pool against its own purchase order. The whole subsystem was built with extensibility in mind: adding a usage-based tier, a teleconsult add-on, or a multi-site B2B operator package is a configuration change against the entitlement service, not a code release.
ArgoView ships as a single web application serving clinics across the United States and the European Union. The English-language build is in production with clinics in California, New York, Texas, Florida, and Washington in the US, and with operators evaluating it in the Netherlands, Germany, France, Ireland, and Sweden in the EU. Region selection is handled by the storage tier rather than the front-end code — the same React application talks to either an EU or US data tier depending on the operator's data-residency choice. Consent and disclosure flows are region-aware: clinics in the EU and EEA receive a GDPR-style granular consent flow for any optional product analytics; clinics in California receive a CCPA-style disclosure in the same flow. Data-handling practices are aligned with GDPR for European users and with the US state-privacy patchwork — CCPA / CPRA (California), VCDPA (Virginia), CPA (Colorado), CTDPA (Connecticut), UCPA (Utah), TDPSA (Texas), and Oregon CPA.
The deployment story is deliberately operator-friendly. Each region's storage tier is provisioned identically from infrastructure-as-code; the application tier is stateless, horizontally scaled, and can be pinned to EU or US regions independently for future data-residency commitments. The product is positioned for HIPAA technical-safeguard mapping for US clinics that need it, and the engineering team behind the build runs a CET workday with East-Coast US overlap (9 AM–1 PM ET) for stand-ups, incident response, and clinical-customer hand-holding during go-lives.
The active custom software development roadmap for ArgoView includes a native iPad capture client for clinics that want offline-first capture in poor-connectivity rooms, deeper PACS interoperability through DICOMweb (QIDO-RS / WADO-RS / STOW-RS), an AI-assisted reporting module that turns captured snapshots into a draft narrative for the clinician to edit, and a multi-tenant operator console for hospital groups running ArgoView across multiple sites. Infrastructure plans include further regionalization across the EU and US, an internal continuous-compliance harness, and a future independent readiness assessment scaffolded into the cloud & DevOps roadmap.
If you are planning a clinical capture platform, a HealthTech tablet product, or any web application where audit-ready PHI handling has to survive an outside reviewer for clinics in the US and EU, we have shipped this stack end to end and can compress the build timeline meaningfully. The engineering team behind ArgoView sits inside YuSMP Group. We work fixed-price for well-scoped MVPs and on dedicated development teams for ongoing delivery, with a CET workday and a guaranteed East-Coast US overlap (9 AM–1 PM ET) window for stand-ups, demos, and incident response.
A clinical capture MVP covering tablet-first recording, patient records, basic scheduling, and a DICOM export to a single PACS typically costs $140k–$280k. Adding HL7 ORU^R01 result messaging, multi-site scheduling, RBAC against an existing identity provider, audit-trail tooling, and HIPAA technical-safeguard mapping for US clinics brings a full-featured product to $320k–$680k. The dominant cost drivers are the DICOM / HL7 interchange work, the PHI hardening pass, and the validation effort against the operator's existing PACS and EMR.
The naive backend-transcode design buffers HD video through a server fleet before the React client sees it, which adds two to six seconds of glass-to-glass latency. That is unacceptable for a clinician steering an endoscope. Browser-tier capture using WebRTC and the MediaRecorder API runs at frame rate, eliminates the transcoder as a single point of failure, and reduces PHI traversal because patient video never hits a third-party transcoding stack. The backend role shrinks to durable storage, indexing, and export.
Export runs as a background pipeline that produces DICOM Secondary Capture objects for still images and DICOM-encapsulated MP4 series for video studies, with HL7 ORU^R01 messages carrying structured results back to the ordering EMR. Each export is signed, hashed, and recorded against the originating study so the chain of custody from procedure room to PACS is auditable. The pipeline supports point-to-point DIMSE in classic hospital environments and is being extended to DICOMweb (QIDO-RS / WADO-RS / STOW-RS) for cloud-native deployments.
ArgoView is GDPR-aligned for European Union clinics, HIPAA-capable for US clinics that map technical safeguards against the product, and acknowledges the US state-privacy patchwork — CCPA / CPRA in California, VCDPA in Virginia, CPA in Colorado, CTDPA in Connecticut, UCPA in Utah, TDPSA in Texas, and Oregon CPA. Patient identifiers are stored in a separate schema joined through opaque rotated tokens, storage is encrypted at rest, every read of a patient record writes to the audit trail, and infrastructure-as-code policies prevent regression.
A focused MVP with browser-tier capture, patient records, a single PACS export route, and a clinic-grade RBAC model typically takes 18–26 weeks. Adding HL7 result messaging, multi-site scheduling, audit-trail tooling, and the readiness work for HIPAA or ISO 27001 mapping adds another 10–14 weeks. The validation pass against an operator's actual PACS and EMR — not the documentation, the live environment — is frequently underestimated and should be budgeted at four to six weeks of dedicated effort.
Related cases
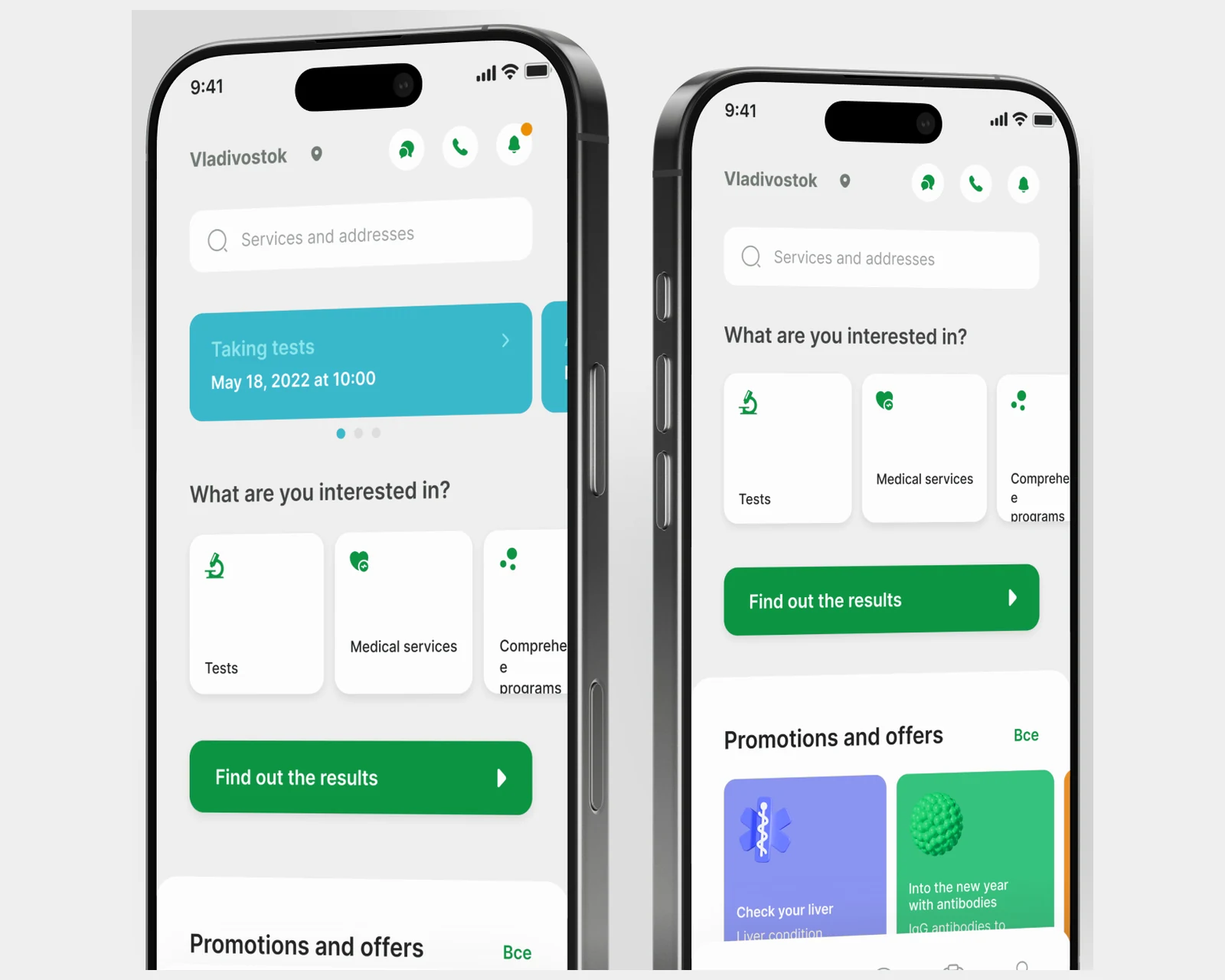
Patient app for a 40-city lab network — appointment booking, digital results, and integrations across the US and EU diagnostic stacks.
View case →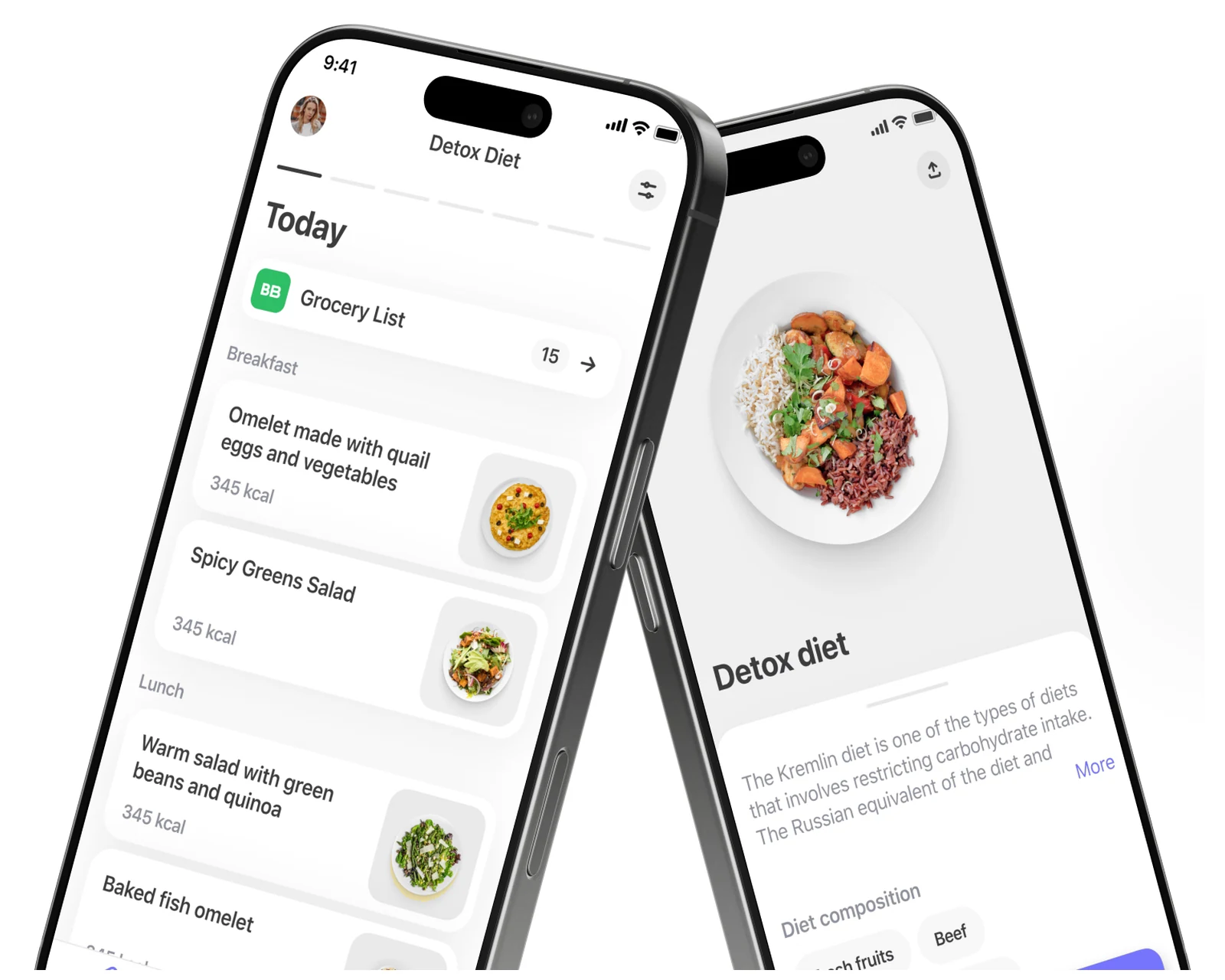
Cross-platform diet and meal-planning app on Flutter — calorie engine, recipe library, grocery ordering for US and EU users.
View case →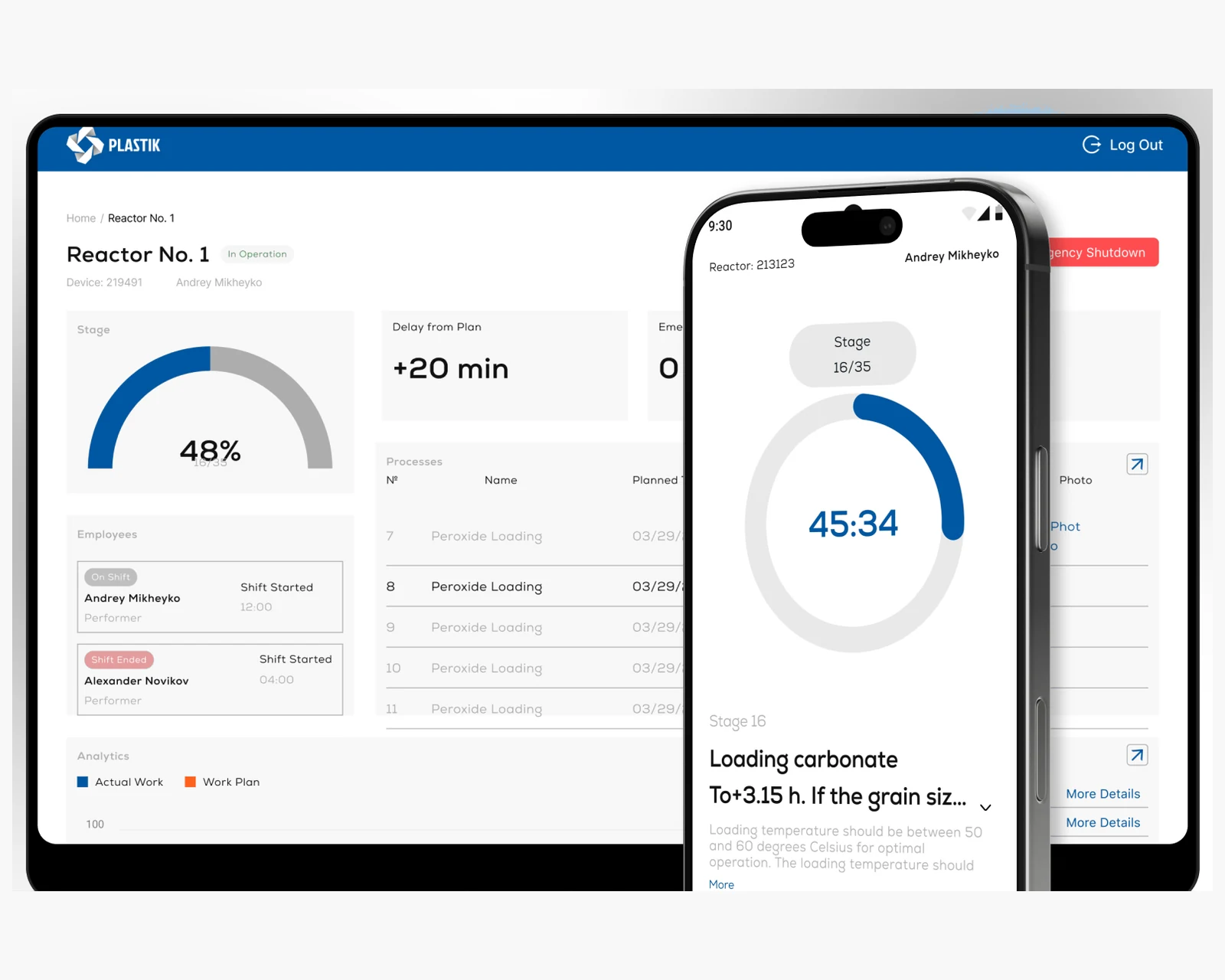
Offline-first ecosystem replacing paper journals for reactor process control — Android, admin, controller dashboard.
View case →Share a few details and a senior consultant will reply within one business day.